Introduction
Shoulder joint is the most movable joint and is also more prone to dislocation than any other joint. It is ball and socket type of synovial joint.
Name the articular surfaces of shoulder joint.
Articular surfaces: Are formed by
- Large round head of the humerus and
- Small and shallow glenoid cavity.
The fibrocartilagenous ring called glenoid labrum deepens the glenoid cavity.
Describe the capsule and ligaments of shoulder joint.
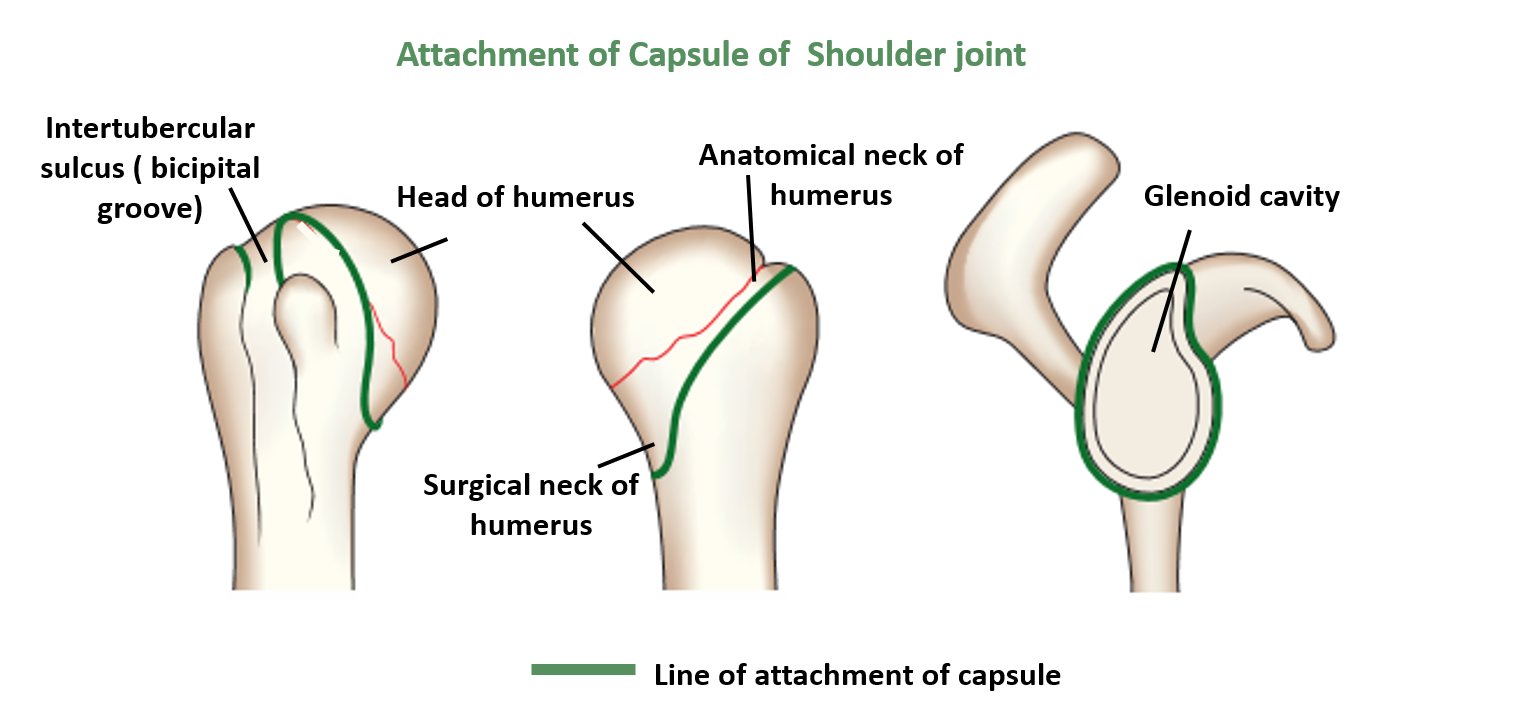
Capsule: The capsule is thick and strong but lax.
- The fibrous capsule surrounds the joint.
- It is attached medially to the margins of the glenoid cavity beyond the glenoid labrum.
- Laterally it attached to the anatomical neck of the humerus except
- Inferiorly where it is attached to the surgical neck of the humerus a finger’s breadth below the articular margin.
- Superiorly at the upper end of the intertubercular groove, it is deficient to allow the passage of the long head of biceps brachii.
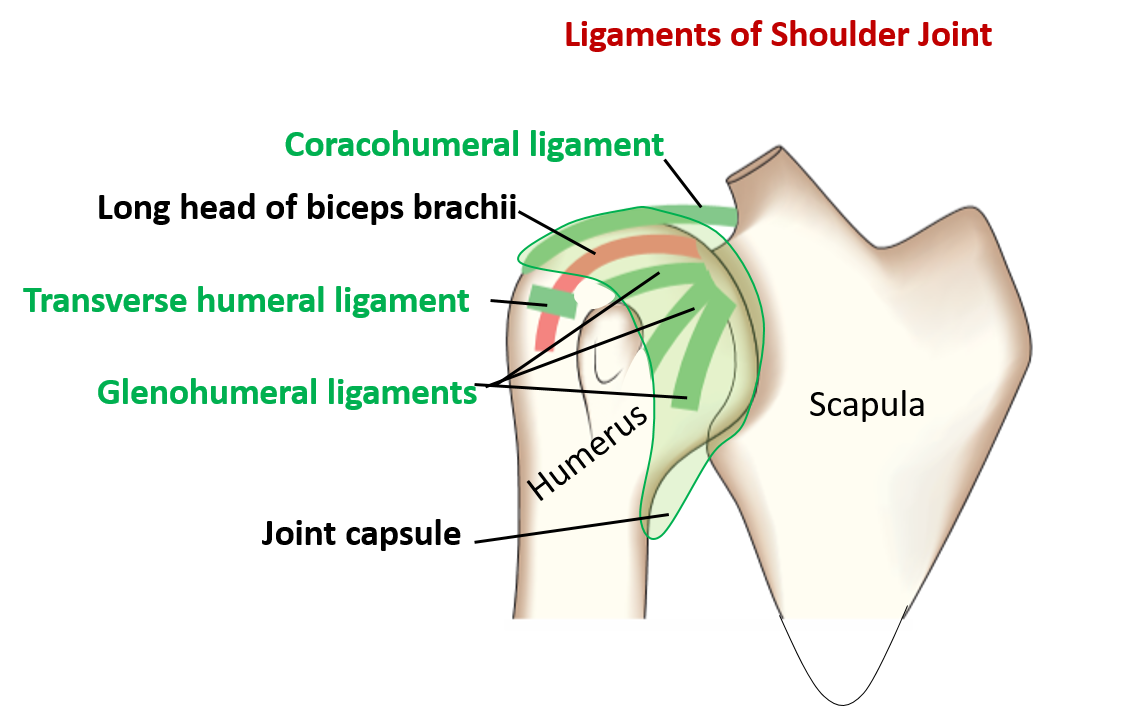
Ligaments:
- Glenohumeral ligaments: Superior , middle & inferior glenohumeral ligaments in the anterior part of the capsule .
- Coracohumeral ligament : extends from the base of the coracoids process to the greater tubercle of the humerus.
- Transverse humeral ligsment : bridges the upper end of the intertubercular sulcus.
Name the factors that provide stability to the shoulder joint.
Factors providing the stability are:
- Muscultendinous cuff/rotator cuff: is formed by the flattened tendons of the
- Subscapularis anteriorly
- Supraspinatus superiorly
- Infraspinatus and teres minor posteriorly
- Coracoacromial arch: prevents the upward dislocation of the head of the humerus.
- Glenoid labrum: deepens the glenoid cavity.
- Long head of biceps brachii: prevents the upward dislocation of the head of the humerus.
(rotator cuff muscles do not support the joint inferiorly)
Name the movements possible at shoulder joint and the muscles responsible for them.
| Movement | Muscles Responsible for the Movement |
|---|---|
| Flexion | Pectoralis major ( clavicular part) |
| Deltoid ( clavicular part ) | |
| Coracobrachialis | |
| Biceps brachii(short head) | |
| Extension | Deltoid (posterior fibers) |
| Latissimus dorsi | |
| Teres major | |
| Long head of triceps | |
| Abduction | 0-15°- Spraspinatus |
| 15-90°- Deltoid (middle fibers) | |
| Overhead abduction: | |
| Serratus anterior | |
| Trapezius | |
| Adduction | Pectoralis major |
| Latissimus dorsi | |
| Teres major | |
| Medial rotation | Subscpularis |
| Deltoid (anterior fibers) | |
| Pectoralis major | |
| Teres major | |
| Latissimus dorsi | |
| Lateral rotation | Infraspinatus |
| Teres minor | |
| Deltoid (posterior fibers) |
Describe briefly the abduction at shoulder joint.
- The first 15 degree of abduction is done by supraspinatus muscle.
- 15-90 degrees is done by deltoid muscle.
- For overhead abduction, the scapula has to be rotated laterally so that the glenoid cavity gradually faces upwards. This is done by upper fibers of trapezius and serratus anterior muscle Every 2 dgrees of movement at shoulder joint is accompanied by 1 degree of rotation of scapula ( called scapulo-humeral rhythm).
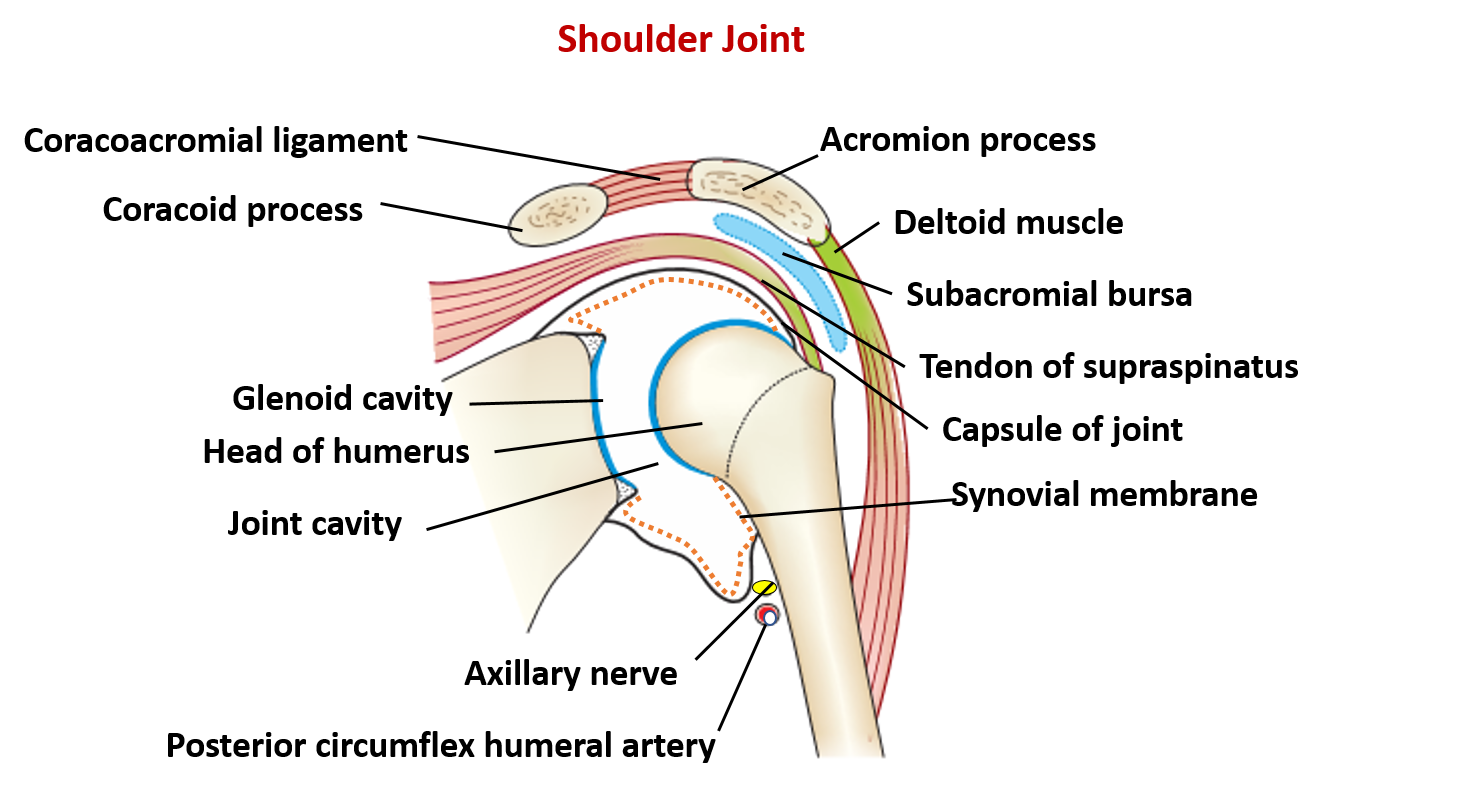
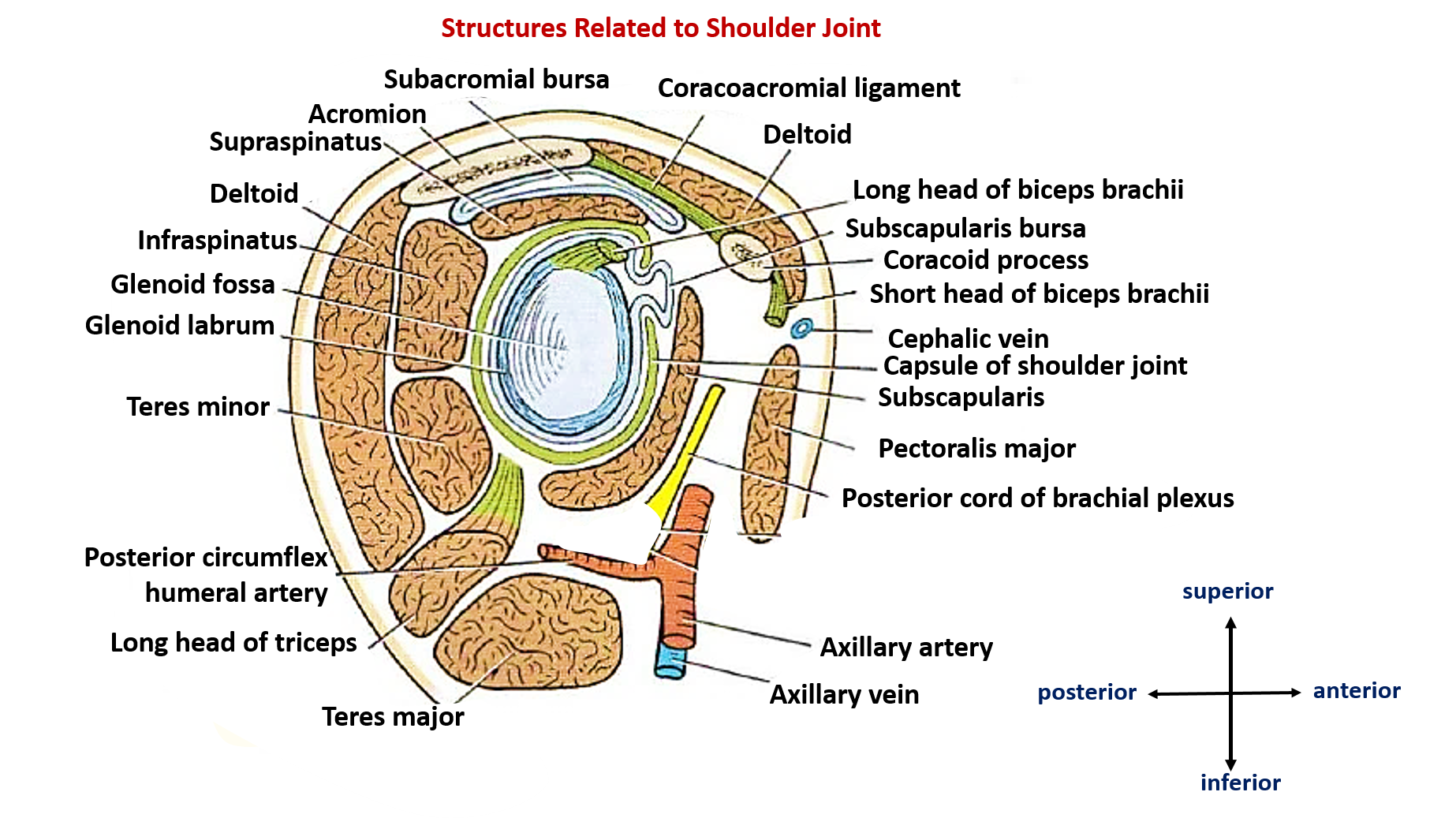
- Relations: the following diagram shows the structures related to shoulder joint.
Draw labelled diagram showing the relations of shoulder joint.
Name the arteries and the nerves that supply shoulder joint.
Arteries supplying shoulder joint
- Suprascapular artery
- Anterior and posterior circumflex humeral arteries
- Subscapular artery
Nerves supplying shoulder joint
- Suprascapular nerve
- Axillary nerve
- Musculocutaneous nerve
Applied Aspects
Inferior dislocation of shoulder joint is common
Inferior dislocation of shoulder joint is common because:
- The capsule descends downwards on the surgical neck inferiorly.
- The capsule is not supported by the muscultendinous cuff inferiorly.
Following inferior dislocation of shoulder joint, the rounded contour of shoulder is lost and there is weakness of abduction of arm.
Following inferior dislocation of shoulder joint, the rounded contour of shoulder is lost and there is weakness of abduction of armbecause the axillary nerve is likely to be injured in the inferior dislocation as it is related to the surgical neck of humerus. As the axillary nerve supplies deltoid muscle, paralysis of deltoid muscle results in loss of abduction (between 15-90 degrees) and rounded contour of shoulder.. Axillary nerve also supplies skin over lower half of deltoid (regimental badge area), therfore sensory loss over regimental badge area is also observed.
Frozen shoulder
Frozen shoulder occurs due to adhesive capsulitis, a disorder in which the capsule and the connective tissue surrounding the shoulder joint becomes inflamed and stiff, greatly restricting movement of shoulder joint and causing chronic pain.
Painful arc syndrome
Thickening or calcium deposits in the supraspinatus tendon or subacromial bursitis results in pain during abduction of shoulder joint from 60° to 120°. This is known as ‘painful arc syndrome‘.